Dielectric ceramics, known for their excellent electrical insulation and mechanical stability, are primarily used in non-bioactive applications, whereas bioactive ceramics, such as hydroxyapatite, promote bone bonding and regeneration by interacting chemically with biological tissues. Bioactive ceramics are preferred for bone implants due to their ability to support osteointegration and accelerate healing compared to inert dielectric ceramics.
Table of Comparison
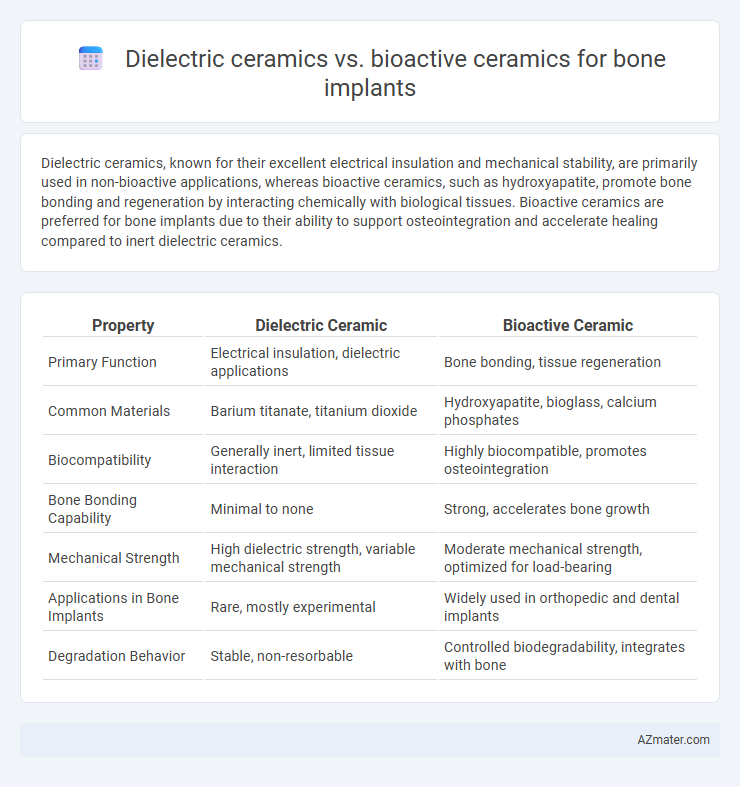
| Property | Dielectric Ceramic | Bioactive Ceramic |
|---|---|---|
| Primary Function | Electrical insulation, dielectric applications | Bone bonding, tissue regeneration |
| Common Materials | Barium titanate, titanium dioxide | Hydroxyapatite, bioglass, calcium phosphates |
| Biocompatibility | Generally inert, limited tissue interaction | Highly biocompatible, promotes osteointegration |
| Bone Bonding Capability | Minimal to none | Strong, accelerates bone growth |
| Mechanical Strength | High dielectric strength, variable mechanical strength | Moderate mechanical strength, optimized for load-bearing |
| Applications in Bone Implants | Rare, mostly experimental | Widely used in orthopedic and dental implants |
| Degradation Behavior | Stable, non-resorbable | Controlled biodegradability, integrates with bone |
Introduction to Ceramic Materials in Bone Implants
Dielectric ceramics, such as alumina and zirconia, are prized in bone implants for their high mechanical strength, electrical insulation properties, and biocompatibility, ensuring structural support in load-bearing applications. Bioactive ceramics like hydroxyapatite and bio-glass actively promote bone regeneration by bonding directly with bone tissue, enhancing osseointegration and healing. Both ceramic types play critical roles in orthopedic implants, with dielectric ceramics providing durability and bioactive ceramics facilitating biological interaction and tissue growth.
Overview of Dielectric Ceramics
Dielectric ceramics, characterized by their high electrical insulation properties and stability under physiological conditions, offer advantageous biocompatibility and mechanical strength for bone implants. These materials, such as alumina and zirconia, exhibit excellent wear resistance and low dielectric loss, making them suitable for load-bearing applications with minimal risk of electrical interference in the body. Unlike bioactive ceramics, dielectric ceramics do not bond directly with bone but provide a durable scaffold supporting bone tissue integration through surface modifications.
Characteristics of Bioactive Ceramics
Bioactive ceramics such as hydroxyapatite and bioglass exhibit strong bonding with bone tissue due to their surface reactivity, promoting osteointegration and stimulating new bone growth. They possess high biocompatibility and bioactivity, enabling the formation of a direct chemical bond with living bone, which contrasts with dielectric ceramics that mainly serve as insulators with limited biological interaction. Their porous structure and controlled degradation rates enhance cell adhesion and proliferation, making bioactive ceramics optimal for bone implant applications.
Mechanical Properties Comparison
Dielectric ceramics, such as alumina and zirconia, exhibit high compressive strength and excellent wear resistance, making them suitable for load-bearing bone implants. Bioactive ceramics like hydroxyapatite and bioactive glass demonstrate superior osteoconductivity and bonding with bone tissue but generally possess lower mechanical strength and fracture toughness compared to dielectric ceramics. The optimal choice for bone implants balances the mechanical robustness of dielectric ceramics with the biological integration advantages of bioactive ceramics.
Biocompatibility and Bioactivity Differences
Dielectric ceramics, such as alumina and zirconia, exhibit excellent biocompatibility due to their chemical inertness and mechanical stability but lack intrinsic bioactivity, limiting direct bone bonding. Bioactive ceramics like hydroxyapatite and bio-glasses possess surface chemistry that promotes osteointegration by forming a carbonated apatite layer, enhancing bone regeneration. The key difference lies in bioactive ceramics' ability to actively stimulate cellular response and bone growth, contrasting with dielectric ceramics' primarily passive compatibility.
Osseointegration Capabilities
Dielectric ceramics exhibit excellent electrical insulation but limited bioactivity, which restricts their ability to promote direct bone bonding and efficient osseointegration in bone implants. In contrast, bioactive ceramics such as hydroxyapatite and bioglass chemically bond with bone tissue, enhancing cell proliferation and accelerating osseointegration through bio-mineralization processes. The superior osseointegration capabilities of bioactive ceramics result in improved implant stability and faster integration compared to dielectric ceramic materials.
Electrical Properties and Their Implications
Dielectric ceramics exhibit high electrical insulation and low conductivity, which limits direct electrical stimulation but provides structural stability in bone implants. Bioactive ceramics, such as hydroxyapatite, possess ionic conductivity facilitating cell signaling and promoting osseointegration through electrical charge interactions. The electrical properties of bioactive ceramics enhance bone regeneration efficiency by stimulating cellular activity, whereas dielectric ceramics mainly serve as passive scaffolds with minimal electrical interaction.
Long-Term Performance and Durability
Dielectric ceramics used in bone implants exhibit excellent electrical insulation and mechanical stability, contributing to their long-term durability under physiological conditions. Bioactive ceramics, such as hydroxyapatite and bioglass, promote direct bonding with bone tissue through biointegration, enhancing implant longevity by stimulating bone regeneration and minimizing implant loosening. The balance between mechanical strength and biological activity determines the optimal choice, with dielectric ceramics favored for structural durability and bioactive ceramics preferred for biological compatibility and long-term osseointegration.
Clinical Applications and Case Studies
Dielectric ceramics, such as alumina and zirconia, are widely used in bone implants due to their high mechanical strength, wear resistance, and electrical insulation properties, making them suitable for load-bearing applications in orthopedic and dental implants. Bioactive ceramics like hydroxyapatite and bio-glass promote direct bone bonding and osteointegration by releasing calcium and phosphate ions, which enhance bone regeneration and healing, proving effective in non-load-bearing defects and coating metallic implants. Clinical case studies demonstrate that bioactive ceramics improve implant osseointegration and reduce healing time, while dielectric ceramics excel in long-term mechanical stability and durability in joint replacements and structural bone repairs.
Future Trends in Ceramic Bone Implant Technology
Future trends in ceramic bone implant technology emphasize the integration of dielectric ceramics with enhanced electrical properties to stimulate osteogenesis and improve bone regeneration. Bioactive ceramics continue to evolve with advancements in surface modification and composite formulations that promote faster osseointegration and biodegradability tailored to patient-specific healing rates. Emerging research highlights the potential of hybrid ceramics combining dielectric and bioactive functionalities to optimize mechanical strength, biocompatibility, and electrochemical signaling for next-generation bone implants.
Infographic: Dielectric ceramic vs Bioactive ceramic for Bone implant